This kidney stone passage calculator uses the physical size of your stone and its location within the urinary tract to estimate the statistical probability that it will pass spontaneously. The algorithm is built upon the established physiological frameworks utilized by the American Urological Association (AUA) and the European Association of Urology (EAU). Not all stones are created equal—a 4mm stone near the bladder has an excellent chance of passing, whereas a 7mm stone high in the kidney rarely navigates the ureter without intervention. Use this tool to generate an evidence-based probability percentage and a printable clinical report to guide the conversation with your urologist regarding conservative management versus surgery.
Key Takeaways
- Size is the ultimate predictor. Stones under 5mm have the highest probability of spontaneous passage. The likelihood drops sharply once a stone exceeds 6mm.
- Location matters immensely. Stones located lower in the urinary tract (the Distal Ureter or UVJ) have already navigated the narrowest sections and are statistically much closer to passing than stones high in the Renal Pelvis.
- Time is a factor. A trial of spontaneous passage typically lasts 2 to 4 weeks. Waiting longer can increase the risk of infection or silent kidney damage.
- Medication can help. Medical Expulsive Therapy (MET), such as alpha-blockers like Tamsulosin, can relax the ureter and improve your odds of passing stones in the 5mm to 8mm range.
In This Guide:
Kidney Stone Passage Calculator
Calculate the statistical probability of a kidney stone passing spontaneously without surgery, based on its specific size in millimeters and anatomical location.
What is the exact size of the stone?
Where is the stone currently located? Look at your CT scan or Ultrasound report. The “Proximal” ureter is near the kidney, the “Distal” ureter is near the bladder, and the UVJ is the final junction right before the bladder.
In My Practice
—
Your Clinical Next Steps
Get Dr. Khalid’s Complete Diet & Prevention Protocol
Enter your email below to receive the free, evidence-based PDF guide on exactly what to eat (and avoid) to stop your next kidney stone from forming.
✓ Copied to clipboard
Retake when you have a new CT scan or imaging report.
What This Tool Measures
This kidney stone passage calculator predicts the statistical likelihood of a stone leaving the body spontaneously, without surgical intervention. It models the two most thoroughly validated predictive variables in endourology: the maximal diameter of the stone in millimeters, and its current anatomical location within the collecting system or ureter. The framework is derived directly from the American Urological Association (AUA) and European Association of Urology (EAU) joint guidelines on urolithiasis management — the same evidence base urologists use when deciding between watchful waiting and operative intervention in clinical practice.
The Physiology of Stone Passage
To understand your probability score, it helps to visualize the journey a stone must make. A kidney stone forms in the collecting system of the kidney. To leave the body, it must travel down the ureter — a muscular tube often only 3 to 4 millimeters wide at its narrowest points. As the stone attempts to pass through this confined space, it stretches the ureteral wall and triggers severe muscular spasms. This is the mechanism behind the excruciating flank pain known as renal colic.
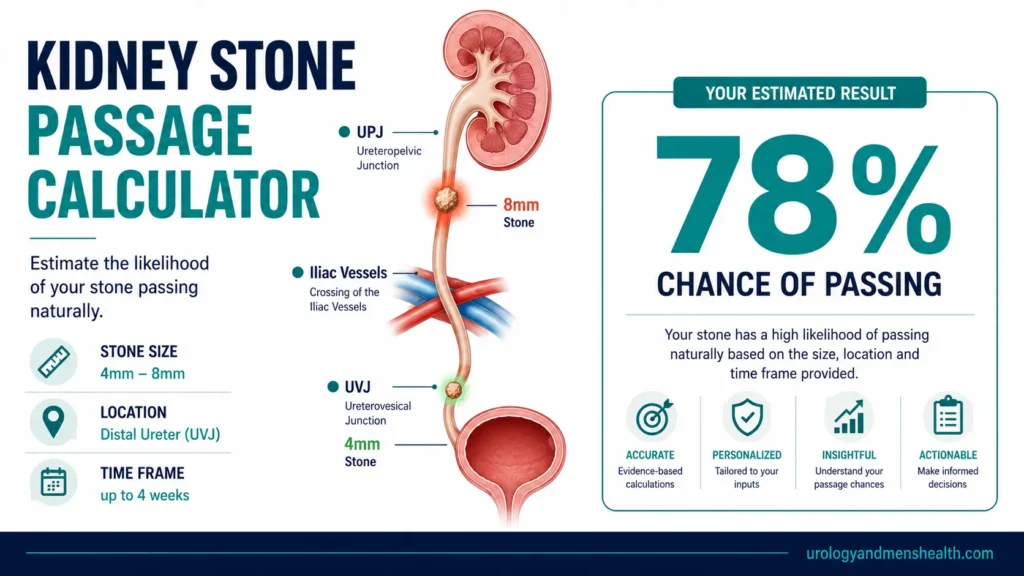
There are three anatomical choke points where stones most commonly become stuck:
- The UPJ (Ureteropelvic Junction): Where the kidney drains into the ureter — the first and often most difficult crossing.
- The Iliac Vessels: Where the ureter crosses over the major pelvic blood vessels mid-course.
- The UVJ (Ureterovesical Junction): The tightest point of all, where the ureter tunnels through the wall of the bladder to reach it.
If your CT scan shows a stone already at the UVJ, you have physiologically navigated roughly 90% of the passage journey. A stone still in the proximal ureter must still negotiate all three choke points.
The 5mm Tipping Point
Five millimeters is the clinical tipping point in stone management. Stones at 4mm or smaller pass spontaneously in over 80% of cases, typically within one to two weeks. Once a stone reaches 5mm the passage probability begins dropping significantly. A 6mm stone is approximately a coin flip — around 50% chance of passage. At 8mm or larger, the probability of passing without urological intervention (Ureteroscopy, Shock Wave Lithotripsy, or PCNL) falls below 20% in most published series.
Related read: Kidney Stone Size Chart — When to Wait vs When to Book SurgeryHow to Interpret and Use Your Result
A High Likelihood result means current AUA guidelines support a trial of spontaneous passage with analgesic coverage and adequate hydration. Medical Expulsive Therapy — typically Tamsulosin (Flomax) 0.4mg at night — can further improve passage rates for stones in the 5 to 8mm range by relaxing ureteral smooth muscle. A Moderate Likelihood result places you in the clinical grey zone: passage is possible but a firm two-to-four-week deadline should be agreed with your urologist, beyond which intervention planning should begin to protect kidney function. A Low Likelihood result means the stone dimensions make spontaneous passage anatomically unlikely; proceeding to a surgical option promptly avoids the risk of silent obstructive nephropathy.
Use the Download My Report (PDF) button below your result to generate a printable two-page clinical summary. Bring this to your urologist appointment — it frames the conversation around your specific stone profile and includes targeted questions to ask about your management options.
Related read: How to Pass a Kidney Stone Fast — Evidence-Based ProtocolIn My Practice
The conversation I have to have most often is with a patient who has been sitting on a 9mm obstructing stone for six weeks, still hoping it will pass. Their GP has been managing the pain, the stone has never moved on repeat imaging, and by the time they reach my clinic one kidney is functioning at reduced capacity from back-pressure hydronephrosis. The stone will not pass — the size makes it physically impossible through a normal ureter. What has happened is six weeks of silent, partially reversible kidney damage that did not need to happen. When this calculator returns a Low Likelihood result, it is not pessimism — it is a prompt to act before that six-week window closes.
A low passage probability score is not a verdict. It is a clinical signal that the most efficient path to resolution is a scheduled procedure, not continued waiting.
Frequently Asked Questions
How accurate is this kidney stone passage calculator?
This calculator provides a statistical estimate based on the two most reliable predictors in urology: stone size and location, drawing directly from AUA and EAU guideline data. No tool is 100% accurate for a specific individual — factors such as prior stone-passing history, ureteral anatomy (including strictures), and stone texture also influence outcomes. It is an evidence-based screening aid, not a substitute for clinical imaging or a urologist’s judgment. For a full clinical picture of what kidney stones involve, read our complete guide to kidney stone symptoms and treatment.
What is Medical Expulsive Therapy (MET)?
Medical Expulsive Therapy uses prescription medications to assist stone passage. The most commonly used drug is Tamsulosin (Flomax), an alpha-1 blocker. Alpha-blockers relax the smooth muscle of the distal ureter, causing it to dilate slightly and reducing the painful muscular spasms that trap the stone. MET significantly improves passage rates for stones between 5mm and 8mm and has a good safety profile for short-term use. It has less clinical impact on very small stones (which pass readily without it) or large stones (which are too wide for the ureter regardless). Learn more in our dedicated guide on Flomax for kidney stone passage.
Does drinking more water push the stone out faster?
Not in the way most people assume. Once a stone is lodged in the ureter, forcing large volumes of water will not “flush” it through — in fact, if the obstruction is complete, excessive drinking temporarily increases the pressure behind the blockage and worsens pain. What hydration does do is keep the urinary tract lubricated, reduce crystallization of new stone material, and maintain urine flow around partial obstructions. Aim for a consistent 2.5 liters (about 85 fl oz) daily rather than periodic large volumes. Read our evidence-based breakdown in our guide to hydration and kidney health.
If the pain stops, does that mean the stone passed?
Not always — and this distinction matters clinically. Sudden pain relief often means the stone has finally dropped into the bladder, from where it passes easily within hours. But pain can also stop because the stone has shifted into a position where it is no longer actively stretching the ureter — it is still obstructing, just silently. Silent obstruction over weeks can cause progressive kidney damage. The only definitive confirmation is catching the stone in a urine strainer or a follow-up CT or ultrasound showing no stone in the ureter. Our kidney stone size chart explains when imaging confirmation is clinically necessary based on stone dimensions.
How do I use this result at my doctor’s appointment?
Click the Download My Report (PDF) button below your result. This generates a printable two-page clinical summary containing your estimated passage probability, your specific stone dimensions, and targeted questions to ask your urologist about conservative management versus surgical options. Hand this to your doctor at the start of the consultation to anchor the discussion on your specific stone profile. Once you have your passage probability, it is also worth assessing your long-term recurrence risk with our 5-Year Kidney Stone Risk Profiler — the two tools together give a complete clinical picture.

Dr. Muhammad Khalid
MBBS · FCPS (Urology) · MCPS (Gen. Surgery) · CHPE · CRSM · IMC #539472
Specialist urologist with 11+ years of clinical experience across tertiary teaching hospitals. Trained at Lady Reading Hospital and Khyber Teaching Hospital, Peshawar. Author of 5 peer-reviewed international publications in Cureus, WJSA, and AJBS. Procedural expertise: URS, PCNL, RIRS, TURP, TURBT, and major open urological surgery. Full profile →
This article is for educational purposes only and does not constitute medical advice. Always consult your physician or urologist for diagnosis and treatment decisions specific to your condition.